
Checking In On Covid Mask Science
Sorry, They Still Don't Work...

It’s been over 18 months now since the pandemic began, which means that many of us are going on nearly 18 months since masks first became mandated in our localities. Here in California, aside from a very brief period during this summer we’ve been under at least a partial mask mandate for well over a year.
You may recall that masks weren’t initially recommended, and it was only after flimsy evidence started to trickle in out of parts of Asia and eastern Europe that all of western science made an about face and started to recommend them. Unfortunately for us, masks didn’t work.
The promise of masks was that they would “flatten the curve” and “stop the spread” entirely. Masks were called the “Indispensable Tool” which could end the pandemic. Let us never forget that over a year ago in July 2020, the former CDC Director Robert Redfield stated if we all wore a mask, “In four, six, eight weeks we could bring this epidemic under control.”
Instead we’ve seen case trends stay remarkably similar with and without masking. All the while the science backing up the mandates has been laughable thin. We’ve seen case studies on hair dressers, masked manikins, and computer models all used to justify masks but harder data has been rare. But that hasn’t stopped the mandates. To the contrary, if anything the push and frenzy for masks may be stronger now than every before.
So I was glad to finally see some interesting science come out that might pin down just how useful (or useless) masks are.
The first was a Cluster-Randomized Controlled Trial on masking out of Bangladesh.
It’s great to finally have one of these. The study randomly selected some villages in Bangladesh to provide with masks and enforced a mask mandate through messaging interventions while other villages went mask-less as a control. This can finally answer the “does my mask protects you?” question that couldn’t be answered by a standard RCT like the Danish Mask Study from last year (which produced a null result aka. masks don’t protect you). So what was the bottom line result of the study?
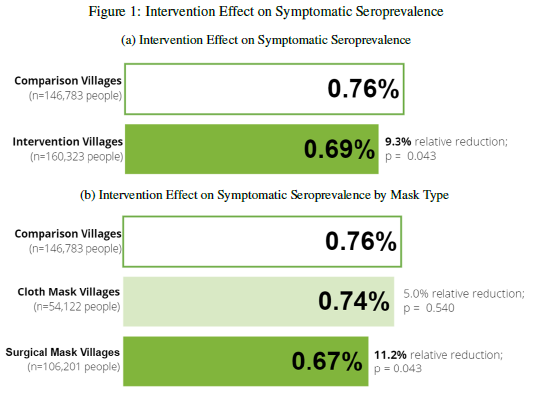
Underwhelming to say the least. They show roughly a 9% decrease in seroprevalence among the masked villages, but the error bars stretch to zero: (adjusted prevalence ratio (aPR) = 0.91 [0.82, 1.00]). It’s a null result for cloth masks, and a barely statistically significant result for surgical masks with the error bars again stretching to zero (aPR = 0.89 [0.78, 1.00]). It actually looks even worse under closer inspection:

A subgroup analysis of seroprevalence by age found no statistical difference at all between surgical mask and control villages for persons under 50 years old. Now, for the higher age groups their was a substantial difference. Persons in their 50’s saw a 23% reduction, and persons aged 60+ saw a 35% reduction. That looks like a substantial benefit, but are we really supposed to believe that masks work, but only once you turn 50? Is there any age specific mechanism which could explain this? No, what is much more likely is that this result is explained by behavioural changes.
The study found 5% higher rates (about a 20% increase) in distancing among all masked villages, specifically 5.3% in surgical mask villages, versus 4.4% in cloth mask villages. In addition to distributing masks, the masked villages all had some combination of extensive communication campaigns including text message reminders, “social signaling”, and insentives for village leaders based on mask compliance. It’s quite possible the entire effect found in this study can by attributed to this communication campaign and the behavioual changes it led to in the elderly.
The study claims it found “clear evidence that surgical masks are effective in reducing symptomatic seroprevalence of SARS-CoV-2”. No! this result would suggest that if masks help at all it’s barely noticable and might be entirely attributable to behavioral changes seen in those who feel most at risk. The masks, coupled with all the messaging interventions, likely just acted as a reminding that the disease was spreading which made those at risk act cautiously and distance more.
This leads to study two, this one a detailed analysis on the physics of aerosol dispersion as it relates to masks and ventilation.
The study measured the accumulation of “exhaled” olive oil aerosols in a sealed room with various masks (or no mask) worn by a CPR manikin. Yes, this is a manikin study, which means it’s not a real world test and doesn’t measure real virus containing aerosols. All flaws, but at least this study was set up to measure accumulated aersols and not simply droplets.
So what did the study find? Under these simulated conditions the study measured filtration efficiencies of around 40% to 50% in cloth and surgical masks versus 95% in KN95 respirators, but as the study noted “a notable amount of particles leak out at the perimeter of all masks, which is expected to result in notably lower effective filtration efficiency, compared to ideal filtration efficiency, when exhalation is considered.” Put another way: Masks Don’t Work…

The end result, was a steady state reduction in aerosols of just 9.8% (+/-9.7% effectively null) in cloth masks, 12.4%(+/-9.7%) in surgical masks. Next to no difference at all from the no-mask control, with the error bars stretching to zero just like in the Bangladesh RCT, and this is before we account for the limitations of the study using olive oil instead of real virus…
Now as for N95 respirators, they can certainly help, and the 45% to 60% efficacy that the study finds for KN95’s and R95’s respectively make sense to me. However, these are "FIT-TESTED" N-95's and that's very important!
As the study shows ( In table III) a KN95 with even a tiny gap (they studied a 3mm gap or about 0.1 inches) is not effective at all! They calculate 3.4% ± 8.9%. Zero!
We perform fit-tests for respirators at my work to prevent silicosis from crusher dust while working at rock crushing plants. To fit test you must be completely clean shaven, with the proper size respirator fitted with no gaps and pressed tightly against your face. It's immediately uncomfortable and hard to tolerate for even 15 minutes, much less 8 hours. If worn repeatedly, the bands around your head and the sides of the mask around your face can cause servere skin bruising. These respirators are not intended for general public use, and you can forget about respirators for kids.

And that's the point. Outside of medical settings where trained professionals are able to wear fit-tested N95's for limited time periods, masks just don't work.
We were told masks were the essential tool to end the pandemic, and they were compared to seat belts and parachutes.

If seat belts were 10% effective they wouldn't be mandated and no one would use them.
If parachutes were 10% effective skydiving would be called suicide.
Yet here we are over 18 months into this pandemic with our Public Health Betters still demanding we all wear face masks, at all times in indoor and somethings even outdoor settings. This includes the youngest among us at no risk from the virus. But masking didn’t work, and now we know why, the science is becoming clearer every day: masks aren’t an essential tool, they are a shockingly ineffective intervention, and we would be better off to ditch them immediately.
Anyway, 0 and 2…
I have no idea what this means "the error bars stretch to zero"